Introduction
Cardiovascular
diseases are one of the most common health problems and one of the leading
causes of death in adults. The presence of cardiovascular risk factors in
childhood and adolescence may lead to long term burden on cardiovascular system
which ultimately results in cardiovascular disease and mortality in adulthood.1
Obesity
which is related to cardiovascular diseases reached epidemic levels in many
countries.2 It is remarkable that the prevalence of childhood
obesity has also increased over the last decades.3
Hypertension
in
childhood
may
become
more
prevalent
than
previously
reported
and
an
epidemiologic
shift
may
be
seen
from
secondary
hypertension
to
primary
hypertension
in
relation
to
increasing
prevalence
of
childhood
obesity.3,4
Many
studies
have
investigated
the
interaction
between
overweight,
hypertension
and
ethnicity.3,5
The
prevalence
of
overweight
and
hypertension
in
childhood
has
increased
among
ethnic
minorities
such
as
Turkish
children
living
in
Netherlands.3,6
There
is
a
recent
study
conducted
in
older
children
in
central
Anatolia.7
However
there
is
no
population
based
study
about
childhood
hypertension
in
Western
Anatolia
where
Mediterranean
life
style
is
more
predominant.
The
aim of this study is to determine the prevalence and predicting factors of
hypertension in primary school students of a Western city, Aydin. .
Material
and
Methods
This
cross-sectional,
descriptive,
population-based
study
was
implemented
between
January-November 2005.
The
study
was
approved
by
Turkish
Ministry
of
Education
and
Local
Ethics
Committee.
Informed
parental
consent
was
obtained.
Study Design and Population
The
sample size was calculated as 1350 children on prevalence of 5%, d=0.05 at a
confidence level of 95%. A design effect of 2 was used to allow for multistage
sampling.8
A
three stage probability design was used to select a representative sample of
primary school children in Aydin between 1st and 8th
grades. Stage one involved to stratify schools by socioeconomic status (low,
medium, high). Total population of schools in each socioeconomic status (SES)
was calculated to have a balanced distribution for SES and gender. In the
second stage, a stratified random selection was performed for total of seven
schools from each SES. In the third stage, one in three students was randomly
selected from each classroom. A questionnaire including demographic information
was filled out for each student. Information was obtained from school records
and from children themselves.
Blood pressure, weight and height
measurements
Mercury
sphygmomanometer was used to measure arterial blood pressure. Bladder with its
width covering at least two thirds of the upper arm and length exceeding 80% of
the biceps circumference was selected for each student. After 10 minute of rest
in a quiet room, three blood pressure and heart rate measurements were taken at
15 minute intervals while student was seated. The average of three measurements
was used in subsequent analysis.
Students
with elevated blood pressure (≥95th percentile) were determined using the
tables provided by the Task Force Report on high blood pressure-specific for
gender, age and height percentile-in children and adolescents.9
Children with an average of three measurements over 95th systolic blood
pressure (SBP) and/or diastolic blood pressure (DBP) percentile considered as
hypertensive.
Weight
was measured in light clothing using a beam balance and height with a
stadiometer. Body mass index (BMI) was calculated as weight (kg)/height
(m)². Determination of overweight and
obesity was obtained by the 85th and 95th percentiles of
BMI for age, respectively, as proposed by Centres for Disease Control (CDC) in
2000.10 Growth curves for healthy Turkish children were used to find
the age-specific height and weight percentile for each student.11
Table 1:
Demographic
characteristics
of
students (n=1348)
|
Demographic
characteristics
|
n (%)
|
|
Gender
Girls
Boys
|
683 (50.7%)
665 (49.3%)
|
|
Parental
education
Mother
Illiterate
Basic reading-writing
skills
Primary
school
Secondary
school
High
school
University
Father
Illiterate
Basic reading-writing
skills
Primary
school
Secondary
school
High
school
University
|
146 (10.8%)
174 (12.9%)
516 (38.3%)
98 (7.3%)
330 (24.4%)
84 (6.2%)
35 (2.6%)
156 (11.6%)
477 (35.4%)
131 (9.7%)
387 (23.7%)
162 (12.0%)
|
|
Occupation
Mother
Housewife
Labourer
(unqualified)
Teacher
Government
officer
Retired
Physician
Other
(housekeeper,
tailor,
etc.)
Father
Labourer
(unqualified)
Tradesman
Government
officer
Unemployed
Security
officer
Retired
Teacher
Farmer
Engineer
Deceased
Other
(shepherd,
hawker,
mechanic,
etc.)
|
1065 (80.4%)
63 (4.7%)
47 (3.5%)
33 (2.4%)
13 (1.0%)
10 (0.7%)
117 (8.9%)
304 (22.6%)
204 (15.1%)
83 (6.2%)
81 (6.1%)
69 (5.1%)
61 (4.5%)
46 (3.4%)
30 (2.2%)
26 (1.9%)
20 (1.5%)
424 (32.3%)
|
|
Body
mass
index
< 85th
percentile
85th -94th
percentile
≥ 95th
percentile
|
1127 (83.6%)
140 (10.4%)
81 (6.0%)
|
|
Socioeconomic
status
Low
Medium
High
|
289 (21.4%)
795 (59.0%)
264 (19.6%)
|
Statistical
Analysis
Descriptive
statistics are presented as percentages, means and standard deviations.
χ2
analyzes was used to define associated factors with hypertension and multiple
logistic regression analysis was used to assess the possible influence of
variables as confounding factors in determining hypertension.
Correlation
between blood pressure and BMI percentile values were analyzed by Spearman’s
rank correlation coefficient. One way ANOVA was performed for between-group
comparisons of categorical and continuous variables. P value <0.05 was used
to indicate statistical significance.
Data were analyzed using the
Statistical Package for the Social Sciences program version 13.0 (SPSS 13.0).
Results
A
total of 1408 primary school students were screened for hypertension. Sixty
children were excluded from the study as four students had heart disease and 56
children had incomplete data. A total of 1348 primary school students were
included in the study.
Mean
age was 10.5±2.4 years. The majority of students were from middle socioeconomic
status. In pre-school period, 1142 (85.2%) children were taken care of by their
mothers and the majority of mothers were housewives. Other care sources were
day-care, grandmother, father and baby-sitter. Demographic characteristics of
children are shown in Table 1.
It
was
remarkable
that
1123 (83.3%)
students
did
not
ever
have
their
blood
pressure
measured
before.
Mean
BMI
percentile
was
48.56%±29.79
and
mean
BMI
was
17.78kg/m2±3.32.
Two
hundred
and
twenty
one
(16.4%)
students
had
BMI≥85th
percentile.
Among
this
group
81 (6.0%)
students
had
BMI≥95th
percentile.
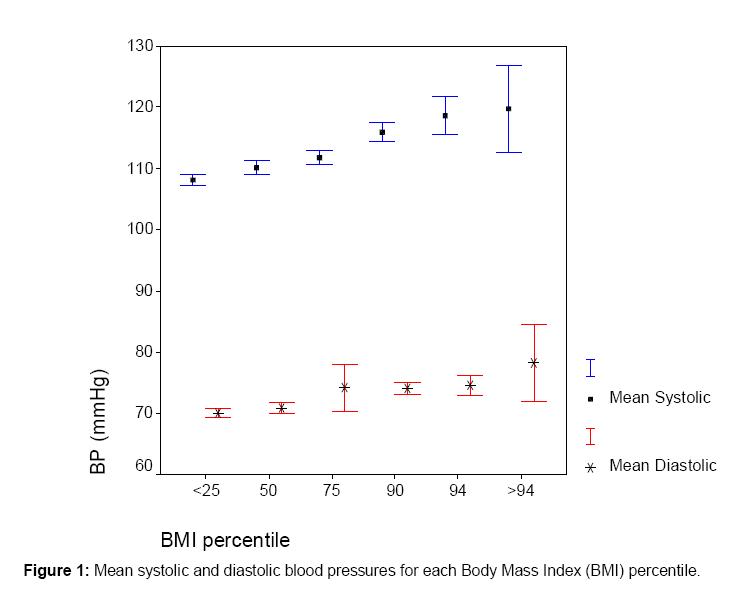
Mean SBP
increased
by
age
(p=0.03)
whereas
there
was
no
significant
change
in
DBP
by
age
(p>0.05).
There
was
significant
increase
in
both
SBP (r=0.323, p<0.001)
and
DBP (r=0.110, p<0.001)
with
increase
in
BMI
percentile.
Mean
SBP
and
DBP
for
each
BMI
percentile
was
shown
in
Figure
1.
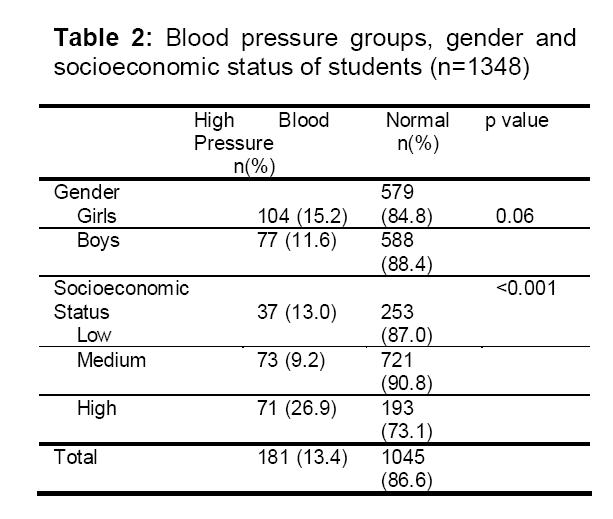
One
hundred and eighty one children had high blood pressure and the prevalence of
hypertension in primary school students was 13.4%. Details of hypertensive and
normal children with regard to gender and socioeconomic status were shown in
Table 2. There was no significant
relationship between hypertension and gender. Results of logistic
regression analysis showed that, obese and high SES students (p<
0.001,
p< 0.001, respectively)
had higher rates of hypertension. Forty-five (24.8%) of the total 181
hypertensive children were either overweight or obese.
Hypertension
and
overweight
and
obesity
were
significantly
high
in
children
from
high
SES.
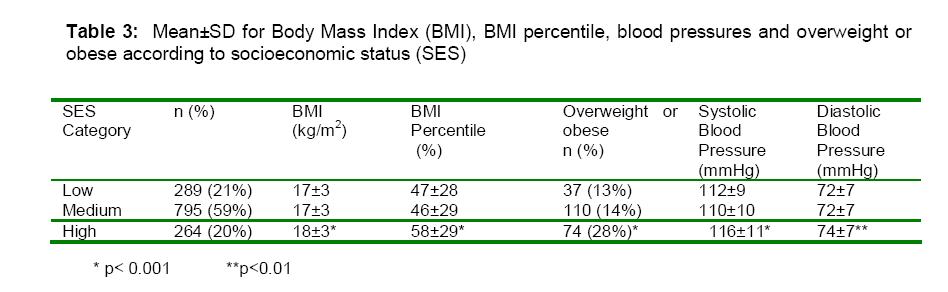
Table 3
shows
mean
values
for BMI
and
blood
pressures
and
proportion
of
overweight
or
obese
according
to
SES.
Discussion
Since
clusters
of
multiple
cardiovascular
risk
factors
persist
strongly
from
childhood
to
adulthood,
screening
children
has
vital
importance
in
detecting
the
risk
factors.
Obesity
is
associated
with
higher
blood
pressure
levels,
various
adverse
biochemical,
physiological,
and
psychological
effects,
many
of
which
have
the
possibility
of
tracking
into
chronic
disease
risk
factors
in
adulthood.12 Studies
have
shown
cardiac
hypertrophy
and
increased
left
ventricular
mass
to
be
associated
with
higher
levels
of
blood
pressure,
which
is
an
independent
risk
factor
for
future
cardiovascular
events
in
adulthood.1
Even
though
age
remains
a
major
determinant
of
vascular
changes,
the
data
from
Bogalusa
Heart
Study
showed
that
approximately
60%
of
overweight
5-10
years
old
children
had
one
cardiovascular
risk
factor,
such
as
high
blood
pressure.1, 13
Hypertension
prevalence
in
screening
studies
of
children
and
adolescents
in
various
age
groups
have
been
recently
reported
in
a
range
between
4.5%
to
23.9%.3,7,14-16
As
an
important
predictor
of
childhood
hypertension,
obesity
in
children
cannot
be
classified
as
a
Western
problem
as
it
is
shared
by
many
industrialized
areas
and
many
developing
countries.12,17-20
Rapidly
increasing
prevalence
of
overweight
and
obesity
even
among
pre-school
children
had
been
reported
from
developing
countries.21
Overweight
and
obese
children
have
significantly
higher
blood
pressure
values
than
normal
weight
children.
Additionally
in
overweight
and
obese
subjects
the
number
of
patients
with
blood
pressure
values
below
the
50th
percentile
was
found
to
be
lower.22 Atabek
et.
al.
reported
in
a
hospital-based
study
that
hypertension
prevalence
in
obese
Turkish
children
was
37.0%.23
Likewise,
Sorof
et.
al.
reported
that
even
though
the
unadjusted
relative
risk
of
hypertension
was
higher
in
some
ethnic
groups,
after
adjustment
for
overweight,
ethnicity
was
no
longer
predisposing
factor
for
hypertension.
Overweight
was
the
strongest
predictor
of
hypertension
in
children.3
Our
findings
were
consistent
with
the
literature.
Girls
have
been
affected
from
overweight
and
obesity
more
than
boys,
and
girls
at
the
85th
percentile
of
BMI
have
begun
to
show
a
marked
increase
of
obesity
after
9
years
of
age.1
Unlike
to
overweight
and
obesity,
gender
was
not
found
to
be
related
to
blood
pressure
level
in
children.24
We
did
not
find
any
gender
difference
with
hypertension
and
overweight
and
obesity.
Socioeconomic
status
is
another
interest
of
point
for
childhood
hypertension.
Conflicting
data
exists
on
the
relationship
between
obesity,
hypertension
and
socioeconomic
status.
Lower
socioeconomic
status
was
reported
as
an
important
predictor
for
increased
prevalence
of
overweight
and
hypertension
in
children
in
developed
countries.19,25
However,
contrary
was
reported
from
developing
countries.17
Likewise,
high
SES
was
associated
with
hypertension,
overweight
and
obesity
in
our
study.
Early
identification
of
children
who
are
at
risk
of
hypertension
is
important
in
preventing
adult
hypertension.
Childhood
hypertension
can
be
identified
easily
by
yearly
measurements
of
blood
pressure
in
all
children
over
3
years
old
in
a
routine
paediatric
well-child
visit
as
recommended
by
Task
Force
on
Blood
Pressure
Control
in
Children.9
Primary
care
centres
are
easily
accessible
and
widely
used
facilities
for
routine
paediatric
well-child
visits.
However,
it
is
unfortunate
that
primary
care
physicians
are
not
sufficiently
detecting,
monitoring
and
managing
hypertension
in
children.1
Furthermore,
with
regard
to
obesity,
an
important
predictor
of
hypertension,
although
the
majority
of
nurse
practitioners
were
aware
of
childhood
obesity
prevention
guidelines,
most
were
not
consistently
using
BMI
for
age
or
monitoring
children
at
increased
risk
for
obesity.26
In
our
study,
it
is
remarkable
that,
%83.3
of
children
between
6-15
years
old
did
not
have
any
previous
blood
pressure
measurement.
New
strategies
should
be
developed
in
primary
care
settings
and
school
health
centres
to
prevent
childhood
hypertension.
Prevention
of disease in childhood is one of the most important goals of primary care, and
success in prevention ultimately will result in reduction of diseases in
adulthood. Primary care physicians and school health workers should play an
important role in childhood obesity and hypertension. They should join forces
between disciplines to mount an effective public health campaign in the
prevention and treatment of these two important public health priorities.
Acknowledgement
We thank
Prof Dr. Ferah Sonmez for her contribution at follow-up stage of hypertensive
children and Dr. Nil Tekin and Dr. Nazli Sensoy for their invaluable efforts in
screening process.
References
1. Berenson GS, Srnivasan SR. For the Bogalusa Heart Study
Group. Cardiovascular risk factors in youth with implications for aging: The
Bogalusa Heart Study. Neurobiol Aging 2005;26:303-7.
2. Crawford D. Population strategies to prevent obesity. BMJ
2002;325:728-9.
3. Sorof JM, Lai D, Turner J, Poffenberger T, Portman RJ.
Overweight, ethnicity, and the prevalence of hypertension in school-aged
children. Pediatrics 2004;113:475- 82.
4. Flynn JT, Alderman MH. Characteristics of children with
primary hypertension seen at a referral center. Pediatr Nephrol 2005;20:961-6.
5. Rosner B, Prineas R, Daniels SR, Loggie J. Blood pressure
differences between blacks and whites in relation to body size among US
children and adolescents. Am J Epidemiol 2000;151:1007-19.
6. Fredriks AM, Van Buuren S, Sing RA, Wit JM,
Verloove-Vanhorick SP. Alarming prevalences of overweight and obesity for
children of Turkish, Moroccan and Dutch origin in The Netherlands according to
international standards. Acta Paediatr 2005;94(4):496-8.
7. Agirbasli M, Cakir S, Ozme S, Ciliv G. Metabolic syndrome
in Turkish children and adolescents. Metabolism 2006;55:1002-06 .
8. Lwanga SK, Lemeshow S. Sample size determination in
health studies: a practical manual. Geneva, World Health Organization, 1991.
9. National High Blood Pressure Education Program Working
Group on Hypertension Control in children and adolescents. Update on the 1987
Task Force Report on High Blood Pressure in children and adolescents a Working
Group Report from the National High Blood Pressure Education Program.
Pediatrics 1996;98:649-58.
10. Department of Health and Human Services: Centers for
Disease Control and Prevention. Available from:
http://www.cdc.gov/nchs/data/nhanes/growthcharts/set1clinical/cj41c024.pdf
and http://www.cdc.gov/nchs/data/nhanes/growthcharts/set1clinical/cj41c023.pdf
Accessed: 29.09.2006
11. Neyzi O, Gunoz H. Buyume ve Gelisme. In: Neyzi O,
Ertugrul T, editors. Pediatri 2nd ed. Istanbul: Nobel Tip Kitabevi; 1993,
63-102 [in Turkish].
12. Sorof J, Daniels S. Obesity hypertension in children: a
problem of epidemic proportions. Hypertension 2002;40(4):441-7.
13. Freedman DS, Dietz WH, Srinivasan SR, Berenson GS. The
relation of overweight to cardiovascular risk factors among children and
adolescents: The Bogalusa Heart Study. Pediatrics 1999;103:1175-82.
14. Lopez-Capape M, Alonso M, Colino E, Mustieles C,
Corbaton J, Barrio R. Frequency of the metabolic syndrome in obese Spanish
pediatric population. Eur J Endocrinol 2006;155(2):313-9.
15. Jago R, Harrell JS, McMurray RG, Edelstein S, El Ghormli L, Bassin S. Prevalence of abnormal lipid and blood pressure values among an ethnically diverse population of eighth-grade adolescents and screening implications. Pediatrics 2006;117(6):2065-73.
16. King CA, Meadows BB, Engelke MK, Swanson M. Prevalence of elevated body mass index and blood pressure in a rural school-aged population: implications for school nurses. J Sch Health 2006;76(4):145-9.
17. Costa RF, Cintra Ide P, Fisberg M. Prevalence of
overweight and obesity in school children of santos city, Brazil. Arq Bras
Endocrinol Metabol 2006;50(1):60-7 [in Portuguese].
18. Hansen
SE, Hasselstrom H, Gronfeldt V,
Froberg K,
Andersen
LB.
Cardiovascular
disease
risk
factors
in 6-7
years
old
Danish
children:
the
Copenhagen
school
child
intervention
study.
Prev
Med 2005;40:740-6.
19. Deckelbaum RJ, Williams CL. Childhood obesity: the
health issue. Obes Res 2001;9 Suppl 4:239S-243S.
20. Hamidi A, Fakhrzadeh H, Moayyeri A, Pourebrahim R,
Heshmat R, Noori M et al. Obesity and associated cardiovascular risk factors in
Iranian children: a cross-sectional study. Pediatr Int 2006;48(6):566-71.
21. De Onis M, Blossner M. Prevalence and trends of
overweight among preschool children in developing countries. Am J Clin Nutr
2000;72(4):1032-39.
22. Schiel R, Beltschicow W, Kramer G, Stein G. Overweight, obesity and elevated blood pressure in children and adolescents. Eur J Med Res 2006;11(3):97-101.
23. Atabek MW, Pirgon O, Kurtoglu S. Prevalence of metabolic
syndrome in obese Turkish children and adolescents. Diabetes Res Clin Pract
2006;72(3):315-21.
24. Tumer N, Yalcinkaya F, Ince E, Ekim M, Kose K, Cakar N
et al. Blood Pressure nomograms for children and adolescents in Turkey. Pediatr
Nephrol 1999;13:438-43.
25. Falkner B, Gidding SS, Garnica GR, Wiltrout SA, West D,
Rappaport EB. The Relationship of body mass index and blood pressure in Primary
Care pediatric patients. J Pediatr 2006;148:195-200.
26. Larsen L, Mandleco B,
Williams M, Tiedeman M.
Childhood
obesity:
Prevention
practices
of
nurse
practitioners.
J
Am Acad
Nurse Pract 2006;18(2):70-9.